Home
Home About Me
About Me Oneironautics
Oneironautics Dream Journal
Dream Journal Academics
Academics Entheogens
Entheogens
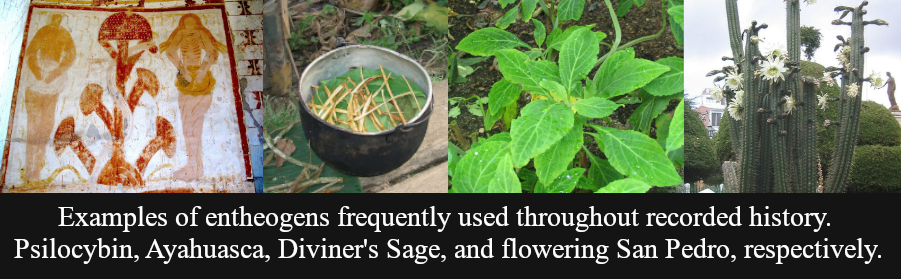
ENTHEOGENS:
Entheogens were a hot topic of debate during my time at Harvard. I will summarize them here for the uninitiated. Please read my page about Oneironautics first if you lack a foundation in that field.
In essence, an entheogen is a mind-altering substance. A psychoactive, a hallucinogen. Your mind is probably already conjuring many examples of such things and you're probably right on the money. The usage of the word entheogen typically includes the context that such a substance is being used in a divine, ritualistic or spiritual setting.
We get the term entheogen from the Greek root "Entheos" which meant to be "full of God, inspired, possessed". When I began my research into the clinical use of entheogens, I believed the "Full of God" part. As I am writing this right now, I suspect that only one part of that definition was correct: "possessed".
You have probably heard stories of yuppie CEOs or hippy weirdoes wandering off into the wilds of South America to indulge in ayahuasca or psilocybin and then just never returning. They go on to become unwashed carnies or drug mules in Cartagena and you never hear from them again. Now you might think me cynical, as there have been clinical studies that show that psychotropic drugs have had positive long term affects for some patients in dealing with trauma and addiction. I don't argue with those claims, as I have not confirmed or disproven them myself. What I do claim, from witnessing it firsthand, is that entheogens leave you vulnerable.
The hallucinogenic state that entheogens induce have been shown to restructure neural pathways and rewire synapses in the human brain. They tear down walls and locked doors that you have built up throughout your whole life. That is why they can be usedful for addictions and trauma. But the problem with renovations like that is that they leave you open to anyone--or anything--just walking in through your wide-open front door.
In the clinical setting, we administered entheogens prior to the patient's sleep cycles, then studied the effects they had on their neural imaging during the dreamstate. We noticed a marked increase in instances of sleep paralysis and nightmares that were strongly correlated with the entheogens administered. Ayahuasca was by far the worst one. Subjects that were administered Ayahuasca experienced night terrors at a near 82% rate and to make matters worse, none of my practiced apotropaic techniques worked on patients under the influence of ayahuasca. So not only would they experience horrible dreamstates, we couldn't do anything to prevent or ease their pain.
If you read my paper about the Importance of Apotropaics in Oneironautics (Located in the Academics section of this webzone) then you will have learned about 'Outer Incidents'. What makes ayahuasca such a dangerous entheogen is that it skyrockets the chances of encountering an 'outer incident'. That isn't to say that all 'outer incidents' are inherently dangerous, but they all have the capacity to be. Allow me to tell you a story to demonstrate what I mean.
Case Study 1982
I am legally required to redact the name of the subjects and researchers involved, but I was once called in to consult on a sleep clinic case in which the patient was experiencing frequent bouts of sleepwalking. As reported by the patient themselves and the notes of the patient's spouse, our patient was experiencing the sleepwalking symptoms on nights in which they had nightmares. Part of our treatment plan involved guided meditation, brain scans for neural imaging, and the administration of certain entheogens in order to provoke a lucid state. We tried several entheogens during the course of our time treating this patient, low-dose ayahuasca included.
Every time we administered ayahuasca to this patient, their personality changed.
On the first night, when we merely observed the sleepwalking in its natural state with no interventions on our part, the patient stood up from their bed, walked clumsily to the table at the center of the room, bumped into it, then woke up.
When we administered ayahuasca, the patient stood up, walked to the table, sat down neatly, folded her hands, and asked for a researcher to enter the room to speak with her. We did not send a researcher in.
We tried this same pattern again on another night and the same thing happened. A polite request to sit with a researcher and speak to them. It occurred two more times, clearly reproduceable. Eventually, I caved and volunteered to be the one to enter the room.
The patient in her waking state was timid, possessed a New Yorker accent, and spoke with a subtle lisp. The sleepwalking patient I sat down with possessed none of those traits. She spoke with a sweet, seductive tone, using all sorts of nicknames and terms of endearment. I asked countless questions and the result was always the same: the person I was speaking to was in no way the waking patient. Toward the end of our conversation, I asked why the "sleepwalker" had wanted to speak with us. It told me that the patient's spouse was abusing her.
We had not had much contact with the patient's spouse during our study, as they lived in a different city from where our clinic was located. There was no evidence at all to confirm that allegation. In fact, the waking patient firmly denied that accusation as well.
It was the decision of the research team's lead (against my advice) to treat the allegation as sleep rambling. The study ended a week later.
Two months later, I received a letter from the sleep clinic. The patient had been murdered by their spouse.
Now the strangest part, the part that still keeps me up at night to this day, is as follows: The patient never sleepwalked again after our study. And when the spouse murdered her, the spouse had been sleepwalking.
I had no clue what to make of any of it. Its the sort of thing that just sweeps all of the science you've ever learned clean off your desk and then asks "Now what?".
One thing was clear to me: if we were going to study lucid dreaming, we needed safeguards. Entheogens were not safe. We needed to be able to control them. And that was where my desire for apotropaic measures began.
Conclusion
My personal recommendation is that if you want to experience lucid dreaming for yourself, then you pursue it without using a chemical agent. Avoid entheogens if you can. There are other methods to achieve a lucid state, such as guided meditation, focused dream journalling, and more. I strongly recommend you pursue those avenues instead. The most pure state of lucidity that we were able to achieve in our studies was always achieved without the use of entheogens. We called it an "Afflatus" state, a pure lucid state akin to opening one's 'third eye'.
It was during afflatus that our patients had the most amount of control of their own perception of the hypnagogic realm. It was during afflatus that chances of 'outer incidents' were reduced. Not eliminated. Reduced. That's a very important distinction.